
Maximize healthcare performance by reducing unwarranted variations
Précis
Hospital financial performance and clinical outcomes are frequently compromised by unwarranted variations, which account for at least 25% of costs. These variations come from diverse sources: some are related to the patient’s condition, the nature of medicine, and the patient’s response to treatment; others stem from the specific training and habits of individual physicians and technicians, and others reside within hospital technology and equipment. The net result is increasing waste in healthcare costs and decreasing quality of care and outcomes. In this article, we describe how a systemic combination of process optimization, leadership, and application of enabling technology lead to reduction of unwarranted variations and individualization of therapy and expansion of precision medicine.
Introduction
In a hospital or other healthcare organization, there are proven ways to reduce unwarranted variations and improve the value of the care provided by the staff. In this article, we identify relevant best practices for healthcare professionals and illustrate them in an actionable 5-step roadmap. The first step in the journey to reducing unwarranted variations is raising awareness within the organization. Success on this journey requires teamwork among executives, clinicians, hospital administration, and staff. Leaders can play an important “coaching” role to champion positive changes in workflows and clinical pathways and to help the staff adjust to and engage with these new ways of working.
Within the continuum of care for any medical condition, the diagnosis phase presents an especially valuable target for reducing unwarranted variations. Specifically addressing evidence-, personnel- and technology-based solutions reduces variations that cause sub-optimal diagnostic performance, which has downstream effects throughout a patient’s journey. This paves the way for care that is both patient-centric and evidence-based while enabling the delivery of precision medicine at scale.
Unwarranted variations: a drag on productivity and performance
The world of sports provides a useful analogy to illustrate the difficulties posed by unwarranted variations (see Figure 1). Athletes obsessively practice their craft. Their dedication to refining their skills is motivated, in large part, by the need to produce consistent, high-quality output by reducing variations. Precise, predictable results from every throw or kick is key to achieving peak performance. Unwarranted variations are limiting factors in the quality of work or performance they can achieve.
In medicine, we have to deal with unwarranted variations as well. These are unnecessary and undesirable differences in patient care—differences that do not arise from medical need, the recommendations of evidence‑based medicine, or patient preferences. By some estimates, 25-65% of all healthcare costs are attributable to unwarranted variations.
The impact of these variations goes beyond cost; they also have a negative impact on clinical outcomes and contribute to a negative patient experience, which itself leads to additional financial losses.
Reducing unwarranted variations is a prerequisite for implementing precision medicine at scale; current variation-prone care delivery practices don’t lend themselves to the standardization and reproducibility that are central to the concept of precision medicine.
Healthcare professionals, supported by technology enablers, can help reduce unwarranted variations without sacrificing the need for personalized medical care.
Where do variations come from?
As we stated earlier, athletes work hard to minimize unwarranted variations for success in their sport. In order to overcome these variations, it’s important to understand their source. Are they the result of bad habits that have been reinforced, a rule change, or new equipment? These variations can only be addressed effectively if the root causes are identified and understood.
The same is true in healthcare, but the difficulty in identifying these sources can be daunting (see Figure 2). The increasing complexity and specialization of healthcare, coupled with the rapid proliferation of new clinical technology, can create a fragmented landscape where standards of care and best practices can vary widely due to extrinsic factors.
Identifying and remedying these variations requires a commitment from both clinical and administrative leadership. The goal is to foster better care at the beginning of the patient pathway and extend that excellence throughout the care continuum.
Key Sources of Unwarranted Variation
With this goal in mind, we present a closer look at some of the most significant sources of unwarranted variations.
1. Craft of medicine: Most physicians see themselves as experts who craft unique diagnostic and therapeutic experiences for each patient, based on their formal education and the subconscious, subjective evaluation of their own practice experience over time. These factors are important sources of unwarranted variations
2. Complexity of medicine: The overflow of new knowledge in medicine, driven by continuous research and discovery, exceeds the capacity of even the brightest clinical mind to absorb and recall when needed.
3. Reduced transparency: Limited access across the healthcare enterprise to evidence-based pathways and peer information, limited digital maturity in the organization, and restricted access to information can make it difficult to establish and share best practices and pathways across a healthcare institution or network.
4.Diagnosis variations: Variations in diagnosis can stem from such factors as device operator bias and skill level that influence results; physician subjectivity can play a major role in how diagnostics decisions are made (as alluded to in point 1); of equal importance, a medical technology may not be adaptable to patients’ individuality and may produce inconsistent results across a hospital fleet as well as across a larger health system
5.(PROPOSED ADDITION) Variation in patient population: Different patients may present similar symptoms but diagnoses of an individual are confounded by age, sex, diet, weight, medications, overall state of health, etc. Further, even when a patient is properly diagnosed, he or she may respond differently to a medication.
Most healthcare organizations have had direct experience with some‚ or all, of these sources of unwarranted variations. Fortunately, solutions to many of these problems have emerged.
Reducing diagnosis variations
Imagine a tennis player with an unreliable, unpredictable serve. The athlete talks to a few coaches and gets a variety of different opinions on what’s going wrong. How can the athlete correct the problem when there are so many competing opinions on what the actual problem is? (see Figure 4)
Key Protocol and Process Steps to Reduce Unwarranted Variations
Similarly, it’s almost impossible to treat a medical condition appropriately without an accurate diagnosis. Incorrect, incomplete, or late diagnoses potentially cause significant downstream costs, because care is delivered under flawed assumptions. With this in mind, let’s take a closer look at how to reduce unwarranted variations in diagnosis.
In the U.S. alone, annual costs due to diagnostic errorshave been estimated at $19.5 billion, with a $13,000 price tag per error.[1] Indeed, every country’s health system pays a substantial price for unwarranted diagnosis variations. Thus, reducing variations early in the care continuum interrupts the cumulative impact of these variations. Here are some key steps that can be taken now to help limit unwarranted diagnosis variations (see Figure 5).
- Achieve consensus on best-practice standards: Evidence-based best practice strategies must be clearly defined, communicated, and enabled, starting at the diagnosis phase. This applies to all other phases of the care continuum; organizational commitment and buy-in from physicians and staff is key.
- Adapt to patients’ individual needs: Every patient is unique, including their anatomy, physiology, and pre-existing comorbidities. Automatically adjusting technology to the specifics of the patient is required for diagnostic consistency. For example, some patients can’t hold their breath, while others can’t take contrast agents; diagnostic medical technology has to adapt to these patient characteristics. Technology that doesn’t adapt to patients leaves us with data that is at best incomplete and inconsistent, and at worst inaccurate.
- Support the device operator through automation: Systems that automate and standardize tasks and pathways (like automatic quality control in a diagnostic device) help to remove operator bias and skill variables from the equation. In addition, automation of routine tasks helps staff work “at the top of their game” by relieving them of repetitive, error-prone procedures. The quality of diagnostic data should be consistent throughout the organization and should not vary based on staff, skill, or time of day.
- Assist decision-making of physician: Choosing the right diagnostic pathway is crucial for generating comprehensive, accurate, actionable information, while reducing waste. Decision support systems can assist the physician by providing context- and patient-specific, easy-to-use, evidence-based information to make informed diagnosis and treatment decisions. They also help produce actionable insights from the vast amount of data available today and can provide context for individual patient’s data.
- Enable reproducibility of technology: Amultitude of diagnostic and clinical data is generated in the diagnosis process. This can lead to cumulative technological variations throughout an institution. Enablers for actively managing diagnostic devices (for availability and updates) and for proactive management (e.g., detecting machines falling out of calibration) improve comparability of results across the organization, preventing variations from happening.
(Quote inset in layout) Getting a handle on consistency in diagnosis gives patients the appropriate start they expect when they enter a care pathway. Addressing these sources of unwarranted variations at the enterprise and the department level requires commitment and teamwork among clinical leadership, hospital administration, and staff.
The leadership playbook for reducing unwarranted variations
Agolfer might feel that she’s got a “hitch” in her swing, compromising her ability to hit the ball with power and confidence. When this occurs, the first step is to identify, characterize, and quantfy what’s happening and how it’s become a problem. It’s often easier for coaches and trainers—as opposed to the athlete herself—to diagnose these individual performance problems because they bring an objective and systematic perspective to the issue.
Key Steps for Hospital Leadership
Similarly, hospital CEOs and their leadership teams can become sponsors, supporters, and coaches in order to identify and correct the unwarranted variations that are limiting the performance of the institution. Hospital leadership is in a unique position to see the overall effects that unwarranted variations have throughout the organization, on patients, and beyond. They can see, for instance, that some care pathways are not delivering the expected clinical and financial results based on benchmark data.
Hospital executives can take a 5-step approach to manage this (see Figure 3):
Create awareness: Raising awareness of unwarranted variations (and their effects) within the institution is a key first step for hospital leadership. As executive sponsors, they can make these effects known and form a coalition of executives, physicians, and nurses to drive sustainable change at the institution. Getting buy-in from clinical and executive teams is key, because addressing unwarranted variations requires ongoing, active participation from both.
- Identify one area of greatest impact: Once the problems have been identified and shared with staff and management, it’s important to identify one or a maximum of two priority issues in order to get some quick “wins.” This will help establish the importance and the effectiveness of this effort. The team will gain confidence and competence when it comes time to implement new processes and pathways.
- Change performance: Healthcare doesn’t stand still, and neither should hospitals. That’s why leadership should establish mechanisms to continually identify variations and implement solutions to tackle these variations and their root causes. That way, initial successes—supported by established and sustainable processes—can be replicated and propagated across the institution on an ongoing basis.
- Build transparency: The right information must be transparent across the hospital. It’s the role of leadership to ensure that clinical decision-makers can have timely access to relevant patient information, as well as to the specific clinical pathways that may yield the best results, so that they can discuss all relevant issues with their patients.
- Expand by leadership and vision: Such change requires inspiration and motivation rather than relying only on directives or mandates. Leaders can get early buy-in from various influencers within the hospital by taking the time to explain the goals and benefits of the program and the ways the team can help achieve those goals for staff, for patients and their families, and for the whole organization.
Conclusion
(Quote inset in layout) Reducing unwarranted variations is a key goal in the larger effort to reduce healthcare costs and deliver higher-value care. There are many sources of variation in medicine, and they are responsible for 25-65% of medical costs. These costs are waste. They destroy value by eroding the quality of care and dramatically increasing the costs associated with that care.
The good news is that unwarranted variations can be identified and addressed through a combination of process optimization, leadership, and application of enabling technology. The way forward is not without its challenges though. Reducing these variations requires a comprehensive and unbiased look at the way each institution operates and embracing the changes needed to improve the situation. Getting buy-in and active participation from clinical and administrative staff is vital to the success of any program designed to reduce unwarranted variations.
Standardized, evidence-based processes for reducing unwarranted variations help healthcare providers deliver precision medicine at scale. Understanding and addressing sources of variations let executives and clinicians focus on what is unique to the patient and their current situation and, consequently, lets the organization focus on delivering the best possible care for its patients.
Author Bios

Luis Lasalvia, MD, MIB
Vice President, Global Medical Officer
Siemens Healthineers
Luis Lasalvia focuses on high-value generation, both clinically and financially. He connects multiple domains in medicine and technology, from innovation and direct clinical practice, into strategy, commercialization, and leadership. He has been keynote speaker, panelist, and moderator at about 500 events and conferences, authored more than 35 papers and articles in peer reviewed journals and other prestigious publications, and submitted multiple patents, He led numerous teams and large enterprise partnerships around the globe, including more than 30 programs in five continents. He’s a medical doctor from the Republic University in Montevideo, holds a Master in International Business from Pompeu Fabra University in Barcelona, and executive education at The Wharton School of Business, New York University, and Harvard Business School

Reto Merges
Global Head of Expanding Precision Medicine
Siemens Healthineers
With more than ten years’ leadership experience in healthcare marketing, Reto Merges has a strong track record in building effective teams for clinical and innovation marketing. In addition, he has four years of work experience in China, ramping up efforts for research collaborations in China and South Korea. Reto Merges holds a degree in electrical engineering and information technology from the Karlsruhe Institute of Technology, Germany, and has studied at the Nanjing Normal University, China. His scientific background is in the field of medical imaging where he has authored many publications, while submitting multiple patents.

Figure 1 Figure 2
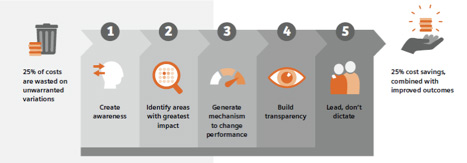
Figure 3
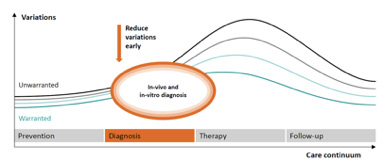
Figure 4
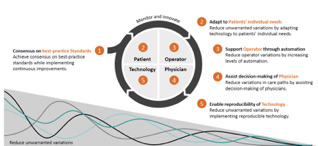
Figure 5
James, B., Lasalvia, L, Merges R. (2019). Insights series – issue 1: 1 Five steps every hospital CEO should start today. Retrieved from https://www.siemens-healthineers.com/insights/news/ insights-series-1.html . (Accessed September 23, 2019)
2 Society to Improve Diagnosis in Medicine. “The Roadmap for Research to Improve Diagnosis, Part 1: Converting National Academy of Medicine Recommendations into Policy Action.” Society to Improve Diagnosis in Medicine, 7 Feb. 2018, www.improvediagnosis.org/wp-content/uploads/2018/10/policy_roadmap_for_diagnosti.pdf. (Accessed September 23, 2019)